

























Overwork and chronic stress can lead many people to having adrenal fatigue as their stress hormones are overused and depleted. This article highlights how it works and how herbal medicines can help.

We see many patients who are distressingly lacking in energy, though perhaps not completely in chronic fatigue, ME, or fibromyalgia territory. The term ‘adrenal fatigue’ was coined in 1998 by a naturopath James Wilson, as a “group of related signs and symptoms that results when the adrenal glands function below the necessary level,” this usually associated with intense stress and often following chronic infections.
However unlike the defined and rare ‘adrenal insufficiency’ (such as Addison’s disease) blood tests do not pick up any reduction in adrenal hormones; to counter this those promoting the adrenal fatigue concept say that this is because these tests aren’t sensitive enough.
Their view is that the body does respond to diminished adrenal function with symptoms such as low energy, brain fog, volatile mood and depression, general aches and pains, food cravings, nervousness, overuse of caffeine and stimulants, sleep disturbances, compromised immunity and/or digestive problems.
The concept has drawn much criticism in conventional medical circles, including on comprehensive methodological grounds (1), although there is a comparable and defined syndrome linked to severe illness ‘Critical Illness-Related Corticosteroid Insufficiency (CIRCI)’ (see below).
Given that ‘adrenal fatigue’ symptoms do arise especially after chronic stress or infection, then it may be better to review what we see and suggest different narratives to help understand the syndrome. Two interpretations will be chosen here: the first is a different biomedical take, the second emerging from many centuries of experience. We can then look at distinctive herbal approaches which have emerged through the different traditions and in particular at the concept of the ‘adaptogen’.
We may conclude that the adrenal fatigue description is inadequate to describe some real and pressing problems, but that there are other more constructive ways to do so.
We will start with an introduction to the adrenal glands.
The adrenals
Adrenal glands, also known as suprarenal glands, are small, triangular-shaped organs on top of both kidneys. They produce hormones that help regulate metabolism, immunity, responses to stressors, fluid balance and blood pressure, and other essential functions. Importantly, there are two distinct parts: the adrenal cortex and the adrenal medulla.
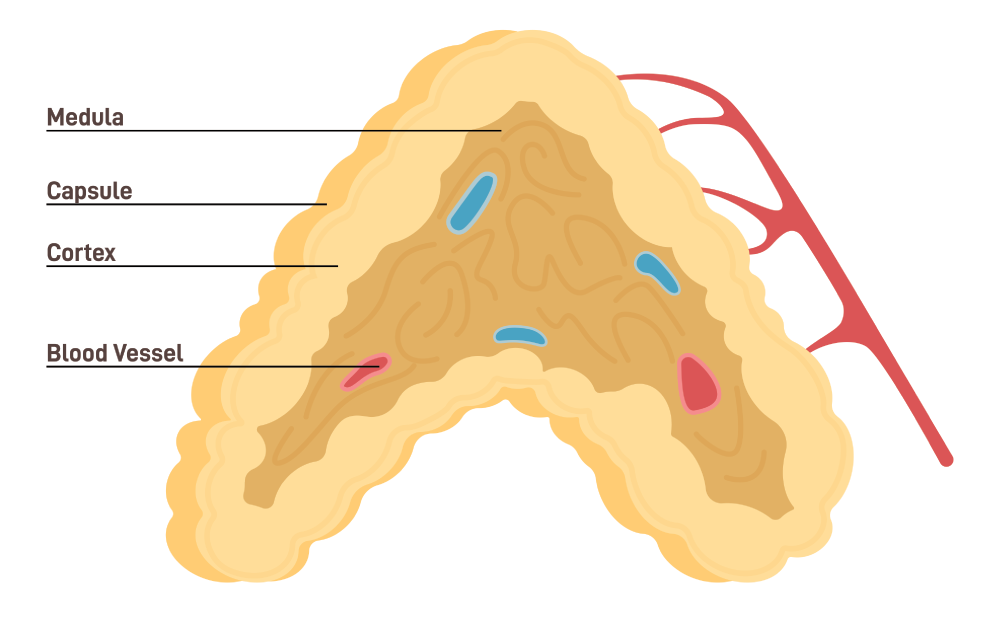
The adrenal cortex is the outer region. It is divided into three zones, each responsible for producing specific hormones.
- Cortisol is a glucocorticoid hormone that plays many important roles in the body. It helps control the body’s use of fats, proteins and carbohydrates; suppresses inflammation; regulates blood pressure; increases blood sugar; and can also affect bone formation. This hormone also controls the sleep/wake cycle. It is released during times of stress to help the body get an energy boost and better handle an emergency situation so it also generates a sense of euphoria.
- Aldosterone is a mineralocorticoid hormone that plays a central role in regulating blood pressure, acidity and the key electrolytes sodium and potassium. It sends signals to the kidneys, resulting in them absorbing more sodium into the bloodstream and releasing potassium into the urine.
- DHEA and the androgens are weak precursor hormones that are converted by the ovaries and testes to augment their own production of oestrogens and testosterone. This link and overlap with the functions of the sex glands is significant (see below).
The adrenal medulla is located at the core of the gland. It is essentially an extension of the sympathetic nervous system and produces ‘fight-fright-flight hormones’ including adrenaline and noradrenaline. This is an almost instant response to alarming situations, especially where urgent extreme physical activity is important, and these hormones increase heart rate and the force of heart contractions, blood flow to the muscles and brain (though in other areas can constrict blood vessels so as to increase blood pressure). They also relax airway smooth muscles to increase breathing efficiency.
So an adrenal stress response has two parts. The immediate reaction to a threat is a flood of adrenaline and noradrenaline from the medulla. The first tissue to be affected by this is the adrenal cortex, which responds in its own way by producing a more sustained response to stress, mainly with cortisol. It is the combination of the two responses that constitutes our adaptation to stress.
Pathologies of the adrenal medulla (e.g. pheochromocytoma) are very rare. There are a number of also relatively rare diagnosable disruptions in function of the adrenal cortex, either primary to the gland or secondary to disorders of the pituitary or hypothalamus.
They include Cushing’s Syndrome, where the adrenals overperform (and can also be a feature of over-prescription of steroids), and Addison’s Disease, which is a severe condition of adrenal insufficiency marked by weight loss, poor appetite, nausea and vomiting, fatigue, darkening of skin and abdominal pain, and can be a feature of potentially fatal ‘adrenal crisis’. The concept of ‘adrenal fatigue’ is not included in the catalogue of medical disorders of the adrenal glands.
The stress response and HPA axis

Modern clinical concepts of ‘stress’ can be traced back to a brief article written in 1936 by the Austro-Hungarian scientist Hans Selye (2). The article set out what appeared to be a three-phase pattern of nonspecific physiological responses to injury: the ‘general adaptation syndrome’: this is made up of 1) an initial alarm phase 2) a stage of accommodation, resistance or adaptation, leading eventually to 3) a stage of exhaustion and even death.
This was a radical and sometimes controversial idea: that many different diseases could have a common cause in the failure of adaptation to stressors, which as well as the physical, such as cold, hunger and infections, could also include emotional and psychological ‘stress’.
It suggested that the body had an exhaustible capacity for coping, that initially it responded to stressors with vitality, learned to manage them for a while, but if the stressors persisted became increasing fatigued.
For Selye steroid hormones lay at the heart of the body’s capacity to adapt to the stress of life: “not only sex,” he wrote in 1949, “but the development and metabolism of the entire body, as well as its resistance and adaptability to exposure and disease, are influenced by the steroid hormones of the gonads, the adrenal cortex and the placenta.”
Although the separate discovery of cortisone as a medicine for the relief of rheumatoid arthritis (which won a Nobel Prize in 1950) were made without reference to Selye’s work, it contributed to a new enthusiasm for the role of steroids and the adrenal cortex in health. It was the linking of the third phase of Selye’s General Adaptation Syndrome with the adrenals that generated the concept of ‘adrenal fatigue’.
However Selye was at least as interested in the wider endocrine system, actually the basis of his most authoritative published works. In particular he led the way in understanding what we now know as the ‘hypothalamic-pituitary-adrenal axis’ (HPA). It is this circuit of the three glands, each producing hormones that regulate and affect the other, that is the real determinant of our adaptation to stress. A well-functioning HPA is an indicator of resilience and coping capacity. Taking into account the hypothalamus and pituitary, and their location as integral parts of the central nervous system, and noting the complex interplay of signals back and forth between the three players (3), is much more useful than focusing just on the ‘adrenals’

Chronic fatigue is one of the syndromes often linked with ‘adrenal fatigue’. A common feature of chronic fatigue syndrome (CFS) appears to be reduced hypothalamic activity with less corticotropin-releasing hormone (CRH); this directly reduces the pituitary’s production of adrenocorticotrophic hormone (ACTH), that in turn reduces adrenal cortex activity (4).
The consequences of underperformance of the HPA axis include disrupted sleep patterns (leading to a vicious cycle of increasing fatigue that exacerbates all CFS symptoms as well as ‘adrenal fatigue’) (5).
There are also pointers to the disruptive role of inflammatory cytokines on the HPA axis (6). This could certainly link adrenal performance to infections, post-viral conditions and chronic inflammation.
However even the HPA role in fatigue is complex and it would be misleading to confine the argument to this endocrine factor alone (7). It is important in making biomedical assessments to remember that there are always wider factors at play. We will return to the ideas of networks later.
The Chinese kidney
A popular synonym for adrenal fatigue syndrome is ‘kidney depletion’, a term appropriated from Traditional Chinese Medicine. The notion is that somehow the kidneys are the body’s powerhouse and that their depletion is analogous to flattened batteries. Not surprisingly, this attribution is even more thoroughly mocked in scientific circles, so before this conversation loses connection with modern experience altogether it is worth taking a look at what the ‘kidney’ means in traditional Chinese thought. The most glaring point is that it means something very different from the modern kidneys!

A general distinction between traditional and modern medical concepts is that the first were induced from cumulative subjective experiences, rather than the dissective, deductive approach that is the foundation of the scientific method. (In the traditional Chinese view dissection was more lowly work, eg. of butchers deconstructing dead bodies, rather than the work of physicians understanding living beings.)
Thus what are assumed as fixed organs in scientific medicine are understood in Chinese tradition as functions (zang fu). In classic texts going back up to 3000 years – like the huang di nei jing su wen -The Yellow Emperors Classic of Internal Medicine (8,9) the Chinese Kidney (shen) is a functional entity (10) that is best understood by reference to our widest experiences of the world.
So the Kidney (shen) is
- linked to the Water phase in the Chinese universal 5-phase cycle and mediates the qualities of water within the living being (sinking, cold, yielding and fluid, tending to stillness, deep and dark, hidden, latent, full of potential, dissolving, necessary for buoyancy/vitality);
- at once the most yin or substantive function in the body: the ‘root of life” (it stores the constitutional energy received from one’s parents), manifest in the deepest tissues: bone and the marrow (which in Chinese observations including the brain and spinal cord);
- but also as the ultimate receptor of inspired vital energy (qi) from the Lungs(fei) it is the source of both yin and yang, water and fire, in the living being, with its yang aspect (ming men huo) the source of body heat and power, the ruler of birth, reproduction and development, the source of our will, and of jing (the vital energy that fuels reproduction and our capacity for action).
One can observe shen as the feeling of fear (which stimulates it to most activity)
- in the health of hair on the head
- in the ears (and hearing)
- in the sound of moaning (or a sad dull voice)
- in sputum
- in the radial pulse: 3rd position on the left (also right) side
- in the bones, teeth, joints and marrow
- when upset as a black hue to the complexion and around the eyes
- in that activity which is supported by moderate levels of bitterness, damaged by excess sweetness and in excess is relieved by moderate saltiness.

So the Chinese Kidney is very much the body’s central resource and powerhouse, manifest in its deepest places and most fundamental functions, including reproduction, birth, and development. There was a certain fatalism about the concept: a large part of Kidney energy is a birthright, to be cultivated by healthy practices, rather than squandered though an excessive lifestyle, and diminution of Kidney energy was seen as mark of ageing itself.
In this context Kidney Deficiency could be seen as potentially terminal and there is no doubt that repleting these energies is the toughest challenge in traditional Chinese therapy.
Although these concepts seem wholly alien to modern medicine there is a fascinating potential correlation between the Chinese Kidney and modern observations, as well as a link to our ‘adrenal fatigue’ theme.
In the human embryo, starting around 4 weeks after conception when it is around a centimetre long, there emerge several important structures in the back of the abdomen. There are primitive and temporary kidney structures, including the mesonephros, which fades away before the final kidney, the metanephros, emerges.
Alongside there is an accumulation of cells that forms the genital (or gonadal) ridge. This ridge develops eventually to form two sets of endocrine glands, the gonads (ovaries or testes) and the adrenal cortex – the only tissues in the adult body that produce steroid hormones.
It is tempting to see a correlation between the embryonic genital ridge and the Chinese Kidney. The experiences that generated the concept of shen are mediated physiologically by the glands that originate in that ridge, which similarly sustain potency and resilience as well as sex and reproduction.
It is a happy coincidence that the course of the genital ridge in the embryonic abdomen is close to the Kidney meridian in the adult. (I am indebted to Richard Cone, Johns Hopkins Emeritus Professor of Biophysics for sharing the conversation that inspired this insight).
A revised approach to adrenal fatigue?
Although not biomedically supported the term ‘adrenal fatigue’ does describe an experience that is not uncommon, and which can be very distressing and disabling, not least because it is poorly explained and there are no useful prescriptions to treat it. This review has picked out different ways to understand the condition, but physiological mechanisms remain elusive. In some ways adrenal fatigue overlaps with chronic fatigue syndrome (see Fatigue) and can be seen as one aspect of this equally challenging condition.

There is one similar but relatively well and authoritatively described syndrome: ‘Critical Illness-Related Corticosteroid Insufficiency (CIRCI)’ associated with severe illnesses. It includes a complex dysregulation of the HPA axis, the suppression of cortisol-metabolizing enzymes in the liver and kidney, leading to raised cortisol levels, and tissue resistance to glucocorticoids (11). Heightened inflammatory activity is identified as a major driver for these disruptions and there may be some overlap with the more chronic conditions we have been discussing here.
Rather than looking for particular biomedical (or psychological) causes of adrenal fatigue syndrome (or any other chronic fatigue pattern) perhaps a more effective approach is to view it as a system breakdown, a failure in the normal self-organising adaptive network of functions in the body. Here a healthy emergent self-organising network of functions becomes chaotically disruptive (12).
The advantage of such a perspective is that rather than chasing elusive single causes, the search is on for ways to reprogram (‘reboot’) the whole system and to identify factors driving the disruptions. For example it has been found that it is helpful to switch the narrative in the management of fibromyalgia from damage and pain to the idea that the body is ‘a very, very clever computer’ where fibromyalgia is caused by a software rather than a hardware problem, by the body adapting when people have to ‘keep going’ despite ‘stop signals’, such as pain and fatigue.
This provides a rationale for engaging in interventions to reprogram the body’s software (13). Taking the opportunity of herbal treatment sessions to construct a ‘rebooting’ programme in which herbs support a strategic reconstruction of coping performance remains one of the best approaches to ‘adrenal fatigue’.
There is ample evidence that syndromes like these involve disturbances in the HPA axis (14), but a wider and more consistent pattern, such as described in CIRCI above, is the increased evidence of inflammatory and immunological activity (15), especially when this also becomes neuroinflammation (16), and in depression also (17). There is some indicative evidence of the benefits of anti-inflammatory diets in managing fatigue syndromes generally (18).
Herbal approaches to adrenal fatigue
Given the absence of useful pharmaceutical approaches to syndromes identified as adrenal fatigue (although one unintended potential benefit of using antidepressants is that they actually down-regulate inflammatory processes (19) there is plenty of opportunity to consider more wholistic herbal solutions that can emerge from traditional insights, and take into account adaptive network ideas.
Certainly a first aim must be to hunt down any possible sources of inflammation, as the most likely driver of the system breakdown. There may already be evidence of chronic inflammatory conditions but these themselves may not be the origin. It is always a good start to assume that inflammatory pressures start in the gut, with increasing evidence of microbiome involvement and there are other Insight pieces in Herbal Reality that pick up on these themes. Look for possibilities of stealth pathogens as causes of chronic inflammatory pressures, those that evade defences and prescriptions and which best be managed by upregulating immune defences.

Setting up a proper convalescence programme is almost always productive as it gives the patient the opportunity to learn how to get on top of the conditions that worsen the exhaustion, like managing sleep, rest, activity, and diet.
Herbal tonics are the obvious first call. They have been poorly defined, with different meanings in different contexts. In this text they refer to remedies that support healthy functions. On one hand remedies used as tonics overlap wholly with foods: different parts of the oat, wheat, barley, rye, asparagus and artichoke, for example, have been used as both foods and medicines. In modern times dietary supplements like evening primrose oil and grape seed have further blurred the distinction.
Other tonics are more dynamic, notably some of those used in Chinese medicine, particularly the yang tonics like fenugreek and eucommia and the qi tonics like Panax ginseng (Asiatic ginseng): these can become a bit stimulating in the very debilitated. A particular application of tonics is to encouraging sleep, lack of which is notoriously part of a fatigue vicious cycle. Tonics like valerian, St John’s wort and notably ashwagandha (see also below) can often help break that cycle by helping charge up the particular sleep batteries.
However by definition the most appropriate herbal approach to supporting adaptation is the ‘adaptogen’. In currently the most definitive review (20), Alexander Panossian and his illustrious co-authors define adaptogens as ‘a category of herbal medicinal and nutritional products promoting adaptability, resilience, and survival of living organisms in stress’.
They emphasise that the term is related to a physiological process—adaptation to environmental challenges, including diverse mechanisms of extracellular and intracellular interactions that fit in well with the network theory above. The paper reviews many adaptogen candidates starting with Schisandra chinensis which inspired the concept in the USSR in the 1950s, initially to improve attention and endurance among the Soviet Armed Forces and the new cosmonauts.
Other adaptogens quickly became official medicines in the USSR: Aralia elata, Eleutherococcus senticosus, Panax ginseng, Oplopanax elatus, Rhodiola rosea, and Rhaponticum carthamoides.
Key points of the adaptogenic concept are in line with basic principles of traditional Asian medical systems like TCM, Japanese Kampo, and Ayurveda, for instance, an assumption is that their tonics, restorative remedies or rasayanas share normalizing effects, irrespective of the nature of the disease.
Ayurvedic rasayanas that are considered as having adaptogenic properties include
- Amla (Emblica officinalis)
- Ashwagandha (Withania somnifera)
- Guduchi (Tinospora cordifolia)
- Haritaki (Terminalia chebula)
- Kalmegh (Andrographis paniculata)
- Pipul (Piper longum)
- Shatavari (Asparagus racemosus)
- Tulsi (Ocimum tenuiflorum. O. sanctum)
- Yasthimadhu (Glycyrrhiza glabra)
Among around a hundred remedies in total listed in the Panossian paper traditional Chinese tonics that particularly fit the adaptogenic definition include
- Bai shao (Paeonia lactiflora)
- Bai zhu (Atractyloides macrocephala)
- Chai hu (Bupleurum falcatum)
- Chuan xiong (Ligusticum wallichii)
- Dang gui (Angelica sinensis)
- Di huang (Rehmannia glutinosa)
- He shou Wu (Polygonum multiflorum)
- Huang qi (Astragalus membranaceus)
- Ren shen (Panax ginseng)
- Suan zao Ren (Zizyphus jujuba)
- Yuan zhi (Polygala tenuifolia)
There are also holistic tools and lifestyle choices which can ease adrenal fatigue. In this article on fatigue, under holistic solutions the knowledge is shared on how to care for oneself beyond herbal treatment.
References
Morris G, Anderson G, Maes M. (2017) Hypothalamic-Pituitary-Adrenal Hypofunction in Myalgic Encephalomyelitis (ME)/Chronic Fatigue Syndrome (CFS) as a Consequence of Activated Immune-Inflammatory and Oxidative and Nitrosative Pathways. Mol Neurobiol. 54(9): 6806-6819.







{kind=link}