

























Racial bias is embedded in the foundations of clinical practice, from imagery to diagnostic tools, requiring practitioners to move beyond awareness toward decolonisation and active anti-racist practice.
What is racial bias?
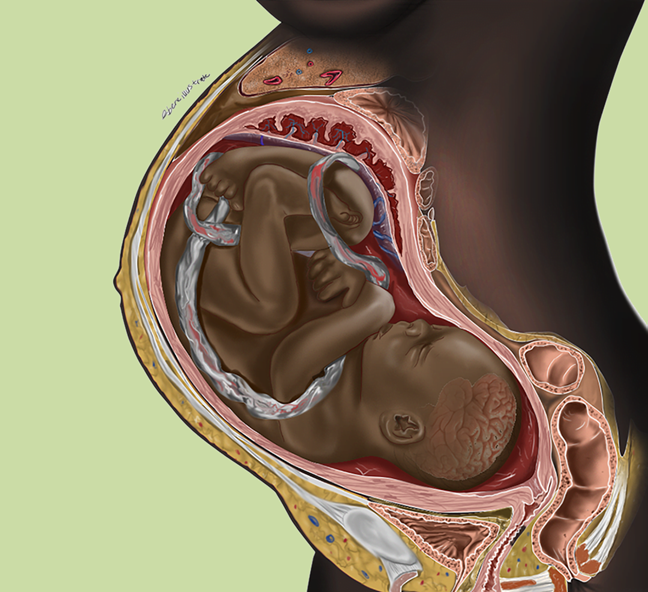
In 2021, Chidiebere Ibe’s medical illustration of a Black foetus in the womb went viral (1,2). It alerted people to acknowledge that while the image may be familiar, this was the first representation many people had seen that wasn’t white. Global attention was drawn to the heavily skewed representation of conditions being primarily depicted on white skin, even in Black majority countries.
This wider recognition made the invisible visible: the inherent racial bias within healthcare.
Race is a socio-political construct with no biological basis (3–5).
Racial bias refers to systemic, institutional and individual prejudices, both conscious and unconscious, implicit and explicit (5–7). These are deep-rooted in institutional structures, societal norms and cultural assumptions. In clinical practice, racial bias manifests not only through overt discrimination but in what is taught, what is seen, who and what is believed.
To understand racial bias we must first examine the perspective from which it operates. Clinical training, whether herbal or conventional biomedicine, reflects the historical Eurocentric white gaze positioned as neutral and universal. It assumes white patients and practitioners as ‘the norm’. Whiteness is presented as the default experience, everyone else becomes ‘other’. This is systemic and institutional, and remained largely unexamined until recent years.
To illustrate how racial bias is embedded in clinical practice, the following sections examine the visual gap in diagnosis, the physiological impact of systemic racism through the Weathering Hypothesis, the limitations of dietary advice, and racial bias within the herbal educational context.
Visibility: Diagnosis on darker skin
Pale skin has been the global default for medical training, a visual example of how implicit bias is ingrained in education and clinical knowledge. Ibe’s viral illustration highlighted the urgent need for diverse representation for patient safety, professional knowledge and for practitioners and patients alike, to see themselves represented and valued.
Dermatology resources for melanated skin are lacking, leading to reduced confidence in recognising conditions. This results in missed and delayed diagnoses, impacting timely access to appropriate care.

Research published in 2026, revealed that resources for Lyme diagnosis are rarely depicted on darker skin, with no images evident before 2020 (8). The study itself misuses the Fitzpatrick scale, a Eurocentric measurement created in 1975 with four white skin tones to assess the propensity for burning during phototherapy.
A further two categories were tacked on later but do not adequately cover the much wider variations of pigmentation in Black and Brown skin (9). The scale was never intended to represent skin tone but is often sampled in this way. False myths around Black skin persist, including the erroneous belief it is immune to burning (as suggested by the Fitzpatrick scale) or developing skin cancer.
The damaging and persistent myth that Black skin is thicker and therefore more resilient to pain remains a legacy of slavery, where dehumanisation sanctioned violence (9). This narrative is countered by the resistance of enslaved people like John Brown whose personal account describes his refusal to display emotion or pain during brutal punishments and pseudo-scientific experiments designed to measure the physiological resilience of ‘the negro’ or gauge the depth skin pigmentation (10).
Inflammation is often described as ‘redness’ with an accompanying image on white skin. On Black skin, inflammation appears darker than the surrounding skin (9,11).
Cyanosis, jaundice, anaemia may be missed because they do not appear blue, yellow or pale on darker skin. Rashes, eczema and psoriasis may not appear red and will look different on melanated skin. Psoriasis may look silvery grey, while eczema can look purplish. Recent outbreaks of scarlet fever and meningitis again highlighted the gap in published visual resources with potentially fatal results. Conversely, Black skin is overrepresented in images of sexually transmitted infections, amplifying harmful racial stereotypes (9,11).
The white default extends to plasters, bandages, joint supports and medical aids. While a ‘flesh’ tone is readily available, it is incredibly difficult to source in any other skin tone than beige. Similarly, the transdermal contraceptive patch still only comes in ‘light nude’ (12). The psychological effect of this indiscreet visual insult on Black skin cannot be underestimated.
These examples illustrate how racial bias is systemic and institutional throughout healthcare and is also the foundation of herbalist curriculums. As resources become increasingly available, they must be integrated into education and not treated as separate add-ons.
Physiology of racism
The health disparities affecting Black and Brown people are not biological differences, but the result of histories of extractive colonialism, displacement, generational trauma and continual systemic racism (6,13,14). Scientific and medical racism persists through racial reference ranges derived from eugenics and slavery. Categories like ‘Black’, ‘Afro-Caribbean’ or ‘Asian’ are treated as homogenous, ignoring diverse ethnicities, and mixed heritages. Studies attributing certain conditions as more prevalent in Global Majority people omit social, environmental and economic contexts, and fail to assess whether the same experience is reflected in Black or Brown majority countries.

This bias is embedded in diagnostic tools. Spirometry (lung function), for instance, only adopted race-neutral references in 2022 (15). Prior to this, adjustments were automatically applied to people identified as Black or Asian, a practice tracing its roots directly to enslavement: “…the expansibility of the lungs is considerably less in the black than the white race … The deficiency in the negro may be safely estimated at 20 per cent…” Cotton is king, and pro-slavery arguments (1860) (16).
Similarly, eGFR (kidney function) calculations were arbitrarily applied to anyone of ‘Afro-Caribbean’ heritage, based on the racist assumption that higher creatinine levels seen in a group of Black Americans were due to higher muscle mass (17). Another throwback to slavery and stereotyped perceptions of the Black body.
These adjustments masked poor lung and kidney health, normalising lower function, resulting in the catastrophic impact of Black people being denied transplants or appropriate treatment until disease was more advanced (17). With eGFR and spirometry ranges only recently updated in 2021 and 2022, many patients are still navigating the consequences.
Beyond diagnostic tools, the physiological toll of systemic racism remains. The experience of living under implicit and explicit racism creates chronic stress in the body, increasing allostatic load (13). Many Global Majority people carry transgenerational and intergenerational collective trauma stemming from colonialism and systemic oppression, displacement from war, genocide, natural disasters and racism. Historical trauma is biologically embedded in the cells of descendants (18,19).
Dr Arline Geronimus coined the Weathering Hypothesis to explain how health disparities are a direct consequence of the cumulative impact of lived and historical trauma and racism (19, 20). This is compounded by resultant socioeconomic disadvantage and is particularly prominent in people racialised as Black and socialised as women (21).
Recent studies in Black Americans and UK Indians confirm elevated allostatic load in these populations (13). Increased chronic inflammation, indicated by higher levels of C-reactive protein, predicts higher rates and earlier onset of chronic disease and autoimmune conditions, such as lupus and diabetes (13,14,21–23).
Diet, lifestyle and the Eurocentric lens

Current dietary guidance often lacks cultural diversity, offering recommendations through a Eurocentric lens. The Mediterranean way of eating is regularly cited as the universal ‘best diet’ while other global traditions are overlooked or even deemed unhealthy.
When people do not see their cultural foods represented in nutritional guides, they do not have the clarity or advice they need with regard to healthy eating. This absence is another layer of racial and cultural bias through erasure.
While herbalists may be knowledgeable about various diets (e.g., vegetarian, vegan, keto, FODMAP), there is generally a lack of formal education on other culinary traditions. This gap means cultural and social contexts are frequently unrecognised, leaving practitioners unable to offer informed, culturally appropriate advice.
Cultural humility involves working collaboratively to modify familiar foods without dismissing or imposing a European standard.
It might be discussions about adapting food preparation or cooking methods, for example, pairing white rice with beans and vegetables to improve glycaemic load rather than eliminating and demonising a staple. It requires understanding the social, familial, religious and cultural roles food plays in someone’s life.
Frameworks for culturally responsive nutrition, such as the toolkit referenced in the resources, offer practical suggestions for a collaborative approach.
Moving forward: Decolonising practice, auditing biases
Educational resources must be actively anti-racist, the absence of racism is insufficient. Herbalists work with a diverse population; anti-racism is essential work for everyone to offer the best, most informed care to all their patients. Practitioners are called to acknowledge and dismantle the systemic biases entrenched in their training. This work is uncomfortable, but necessary, particularly in a climate where tensions are increasing, with rising nationalism intersecting with alternative wellness trends, herbal medicine sits in a complex space.
Herbal education needs to acknowledge the extra mental load Global Majority students carry when navigating predominately white spaces, while their own lived experiences of racial discrimination are rendered invisible in the curriculum. Safety in training clinics cannot be assumed. Clinical trainers need to recognise the weight of systemic racism felt by racialised students, inside and outside the clinic space, implicit and explicit.
Racial bias is multi-directional. Black or Brown herbalists may face patients with fetishised ideas of perceived ‘authenticity’, tribal or mystical connections to the earth, or may encounter more negative racist beliefs. White practitioners, teachers and clinical trainers are encouraged to acknowledge this burden. Anti-racism and decolonisation involves creating safer spaces where students are not forced to educate their trainers while studying, and where power dynamics are navigated consciously.
To achieve this, herbalists are invited to audit their own multiple identities. This could include heritage, class, gender, sexual orientation, disability, age — consider how these intersect and shape assumptions, cultivating curiosity to gaps in experience and understanding. Intake forms could offer open space for self identification of heritage, culture and religion to foster cultural humility and avoid reductive tick boxes or ‘other’. The act of asking enables visibility. Asking about cultural food practices empowers patients through collaboration.
Consider how the current socio-political climate might impact an individual’s health. An audit of resources will reveal gaps in visual references and prompt practitioners to become acquainted with the problematic histories behind herbal and medical practice. Recognising these histories contextualises current policies, ensuring an understanding that these formed the foundations of racial bias in clinical practice. This requires a continual practice of recognising and interrupting implicit or unconscious bias, taking time unlearning and listening to a diversity of voices, re-evaluating and reassessing biases.
Deconstructing racial bias begins with initiating and sustaining these conversations, with the knowledge that a culturally responsive clinical practice is not optional, but essential.
Resources
References
- TODAY.com. Why everyone is talking about this beautiful illustration of a Black parent and fetus. TODAY.com. December 9, 2021. https://www.today.com/health/health/beautiful-illustration-black-parent-fetus-gains-praise-rcna8106. Accessed April 12, 2026.
- Ibe C. Medical Illustrations. Chidiebere Ibe. https://www.chidiebereibe.com/works/. Accessed April 12, 2026.
- Kanwal J. Race is not a biological category: challenging this misconception will help tackle racism in healthcare. BMJ. 2026;392:s150. https://doi.org/10.1136/bmj.s150
- The King’s Fund. Moving from not racist to anti-racist. The King’s Fund. https://www.kingsfund.org.uk/insight-and-analysis/blogs/moving-from-not-racist-to-anti-racist. Accessed March 17, 2026.
- Kaiser Family Foundation. Use of race in clinical diagnosis and decision making: overview and implications. KFF. December 9, 2021. https://www.kff.org/racial-equity-and-health-policy/use-of-race-in-clinical-diagnosis-and-decision-making-overview-and-implications/. Accessed March 16, 2026.
- Catalog of Bias. Racial bias. Catalog of Bias. https://catalogofbias.org/biases/racial-bias/. Accessed March 15, 2026.
- Clinical Tree. Deconstructing racism and bias in clinical medicine. Clinical Tree. March 18, 2024. https://clinicalpub.com/deconstructing-racism-and-bias-in-clinical-medicine/. Accessed March 3, 2026.
- Baffoe-Mensah N, Lipoff JB, Forke CM. Skin tone representation of early Lyme disease in medical education resources: gaps and implications for equity. J Med Educ Curric Dev. 2026;13:23821205251407778. https://doi.org/10.1177/23821205251407778
- Sowomimo A. Divided. Wellcome Collection; 2023.
- Brown J. Slave Life in Georgia: A Narrative of the Life, Sufferings, and Escape of John Brown, a Fugitive Slave, Now in England. University of North Carolina; 1854. https://docsouth.unc.edu/neh/jbrown/jbrown.html. Accessed April 26, 2026.
- Kaundinya T, Kundu RV. Diversity of skin images in medical texts: recommendations for student advocacy in medical education. J Med Educ Curric Dev. 2021;8:23821205211025855. https://doi.org/10.1177/23821205211025855
- Poppe B, Nouri-Nikbakht R, Codd J, Concepcion J, Mercer L, Bond R. Transdermal contraception and reproductive justice: bridging gaps for women of color. NPJ Womens Health. 2025;3(1):51. https://doi.org/10.1038/s44294-025-00102-x
- Marya R, Patel R. Inflamed. Penguin Random House; 2022.
- Simons RL, Lei MK, Klopack E, Zhang Y, Gibbons FX, Beach SRH. Racial discrimination, inflammation, and chronic illness among African American women at midlife: support for the weathering perspective. J Racial Ethn Health Disparities. 2021;8(2):339–349. https://doi.org/10.1007/s40615-020-00786-8
- Tanabe N. Is the Global Lung Function Initiative race-neutral spirometry reference equation ready for clinical use around the world? CHEST. 2025;167(2):303–304. https://doi.org/10.1016/j.chest.2024.10.001
- Pritchard A, Abbott J, Loomis S. Cotton Is King, and Pro-Slavery Arguments. Published 1860.
- Uppal P, Golden BL, Panicker A, Khan OA, Burday MJ. The case against race-based GFR. Del J Public Health. 2022;8(3):86–89. https://doi.org/10.32481/djph.2022.08.014
- El-Khalil C, Tudor DC, Nedelcea C. Impact of intergenerational trauma on second-generation descendants: a systematic review. BMC Psychol. 2025;13:668. https://doi.org/10.1186/s40359-025-03012-4
- Centre for Mental Health. A Constant Battle: Exploring the Intergenerational Consequences of Racism in the UK. Centre for Mental Health; 2023. https://raceequalityfoundation.org.uk/wp-content/uploads/2023/10/CentreforMH_Briefing62AConstantBattleFinal.pdf. Accessed April 12, 2026.
- Geronimus AT. The weathering hypothesis and the health of African-American women and infants: evidence and speculations. Ethn Dis. 1992;2(3):207–221.
- Martz CD, Wang Y, Chung KW, et al. Incident racial discrimination predicts elevated C-reactive protein in the Black Women’s Experiences Living with Lupus (BeWELL) study. Brain Behav Immun. 2023;112:77–84. https://doi.org/10.1016/j.bbi.2023.06.004
- Michel R, Nicholson WK, Borahay MA. The fibroid crisis in Black women: more work to be done! Am J Obstet Gynecol. 2024;231(3):287–288. https://doi.org/10.1016/j.ajog.2024.07.001
- Boston University. Racism, sexism, and the crisis of Black women’s health. Boston University. November 28, 2023. https://www.bu.edu/articles/2023/racism-sexism-and-the-crisis-of-black-womens-health/. Accessed April 8, 2026.



